Novacne
Order generic novacne pillsThis orientation drawing of the alimentary system indicates the final place and relationships of the intestines skin care 11 year olds purchase novacne with paypal. It begins on the pylorus on the best facet and ends at the duodenojejunal flexure (junction) on the left aspect acne prescription medication purchase online novacne. This junction occurs roughly at the level of the L2 vertebra, 2�3 cm to the left of the midline. The junction usually takes the type of an acute angle, the duodenojejunal flexure. Most of the duodenum is mounted by peritoneum to constructions on the posterior belly wall and is considered partially retroperitoneal. The duodenum, pancreas, and spleen and their blood provide are revealed by removal of the stomach, transverse colon, and peritoneum. The stomach aorta and inferior vena cava occupy the vertical concavity posterior to the pinnacle of the pancreas and third a part of the duodenum. The uncinate process is the extension of the top of the pancreas that passes posterior to the superior mesenteric vessels. The bile duct is descending in a fissure (opened up) in the posterior a half of the head of the pancreas. Superior (first) part: brief (approximately 5 cm) and lies anterolateral to the body of the L1 vertebra. Descending (second) half: longer (7�10 cm) and descends alongside the right 1094 sides of the L1�L3 vertebrae. Ascending (fourth) part: short (5 cm) and begins at the left of the L3 vertebra and rises superiorly as far as the superior border of the L2 vertebra. The first 2 cm of the superior a part of the duodenum, instantly distal to the pylorus, has a mesentery and is cell. This free half, called the ampulla (duodenal cap), has an appearance distinct from the rest of the duodenum when noticed radiographically utilizing distinction medium. The superior a part of the duodenum ascends from the pylorus and is overlapped by the liver and gallbladder. The proximal part has the hepatoduodenal ligament (part of the lesser omentum) attached superiorly and the higher omentum hooked up inferiorly. The descending part of the duodenum runs inferiorly, curving across the head of the pancreas. These ducts normally unite to type the hepatopancreatic ampulla, which opens on an eminence, known as the most important duodenal papilla, positioned posteromedially within the descending duodenum.
Discount novacne 5 mg lineThe lateral skin care gift baskets best purchase for novacne, fan-like radial collateral ligament extends from the lateral epicondyle of the humerus and blends distally with the anular ligament of the radius acne y estres discount novacne, which encircles and holds the top of the radius within the radial notch of the ulna, forming the proximal radio-ulnar joint and permitting pronation and supination of the forearm. The fanlike radial collateral ligament is connected to the anular ligament of the radius, however its superficial fibers continue on to the ulna. The ulnar collateral ligament has a robust, spherical, cord-like anterior band (part), which is taut when the elbow joint is extended, and a weak, fan-like posterior band, which is taut 667 when the joint is flexed. The medial, triangular ulnar collateral ligament extends from the medial epicondyle of the humerus to the coronoid process and olecranon of the ulna and consists of three bands: (1) the anterior cord-like band is the strongest, (2) the posterior fan-like band is the weakest, and (3) the slender indirect band deepens the socket for the trochlea of the humerus. The long axis of the fully prolonged ulna makes an angle of approximately 170� with the lengthy axis of the humerus. The obliquity of the ulna and thus of the carrying angle is more pronounced (the angle is roughly 10� more acute) in ladies than in men. It is claimed to enable the swinging limbs to clear the wide feminine pelvis when walking. This angle is made 668 by the axes of the arm and forearm when the elbow is absolutely extended. This is claimed to enable for clearance of the broader female pelvis as the limbs swing throughout walking; nevertheless, no significant difference exists concerning the function of the elbow. In turn, their function and efficiency in the different movements they produce are affected by elbow place. The brachioradialis can produce rapid flexion in the absence of resistance (even when the chief flexors are paralyzed). Normally, in the presence of resistance, the brachioradialis and pronator teres assist the chief flexors in producing slower flexion. The chief extensor of the elbow joint is the triceps brachii, especially the medial head, weakly assisted by the anconeus. Of the a number of bursae across the elbow joint, the olecranon bursae are most necessary clinically. Intratendinous olecranon bursa, which is usually current in the tendon of triceps brachii. The bicipitoradial bursa (biceps bursa) separates the biceps tendon from, and reduces abrasion in opposition to, the anterior part of the radial tuberosity. The anular ligament attaches to the radial notch of the ulna, forming a collar across the head of the radius. The articular cavity of the joint is steady with that of the elbow joint, as demonstrated by the blue latex injected into that area and seen through the skinny elements of the fibrous layer of the capsule, together with a small space distal to the anular ligament. The synovial membrane lines the deep floor of the fibrous layer and nonarticulating aspects of the bones.
Buy novacne without a prescriptionThe rectus abdominis is a strong flexor of the thoracic and especially lumbar areas of the vertebral column skin care and pregnancy purchase generic novacne from india, pulling the anterior costal margin and pubic crest towards one another acne shoes buy 10mg novacne amex. The oblique belly muscle tissue also help in actions of the trunk, particularly lateral flexion of the lumbar vertebrae and rotation of the decrease thoracic vertebral column. The transversus abdominis probably has no considerable effect on the vertebral column (Standring, 2016). The exception occurs on the L1 degree, the place the L1 anterior ramus bifurcates into two named peripheral nerves. Each dermatome begins posteriorly overlying the intervertebral foramen by which the spinal nerve exits the vertebral column and follows the slope of the ribs around the trunk. Iliohypogastric and ilio-inguinal nerves: terminal branches of the anterior ramus of spinal nerve L1. The thoraco-abdominal nerves pass infero-anteriorly from the intercostal spaces and run in the neurovascular aircraft between the inner indirect and the transversus abdominis muscles to provide the abdominal pores and skin and muscle tissue. The lateral cutaneous branches emerge from the musculature of the anterolateral wall to enter the subcutaneous tissue along the anterior axillary line (as anterior and posterior divisions), whereas the anterior belly cutaneous branches pierce the rectus sheath to enter the subcutaneous tissue a short distance from the median aircraft. T11, plus the cutaneous branches of the subcostal (T12), iliohypogastric, and ilio-inguinal (L1), provide the pores and skin inferior to the umbilicus. During their course by way of the anterolateral stomach wall, the thoracoabdominal, subcostal, and iliohypogastric nerves talk with one another. Cutaneous veins surrounding the umbilicus anastomose with para-umbilical veins, small tributaries of the hepatic portal vein that parallel the obliterated umbilical vein (round ligament of the liver). A relatively direct lateral superficial anastomotic channel, the thoraco-epigastric vein, might exist or develop (as a result of altered venous flow) between the superficial epigastric vein (a femoral vein tributary) and the lateral thoracic vein (an axillary vein tributary). The deeper veins of the anterolateral stomach wall accompany the arteries, bearing the identical name. A deeper, medial venous anastomosis may exist or develop between the inferior epigastric vein (an exterior iliac vein tributary) and the superior epigastric/internal thoracic veins (subclavian vein tributaries). The superficial and deep anastomoses may afford collateral circulation during blockage of both vena cava. The major blood vessels (arteries and veins) of the anterolateral belly wall are as follows: Superior epigastric vessels and branches of the musculophrenic vessels from the interior thoracic vessels. Inferior epigastric and deep circumflex iliac vessels from the external iliac vessels. Superficial circumflex iliac and superficial epigastric vessels from the femoral artery and larger saphenous vein, respectively. The distribution of the deep stomach blood vessels displays the arrangement of the muscles: the vessels of the anterolateral belly wall have an indirect, circumferential sample (similar to the intercostal vessels;. It enters the rectus sheath superiorly via its posterior layer and supplies the superior a half of the rectus abdominis and anastomoses with the inferior epigastric artery roughly in the umbilical region. The inferior epigastric artery arises from the external iliac artery simply superior to the inguinal ligament. It runs superiorly in the transversalis fascia to enter the rectus sheath under the arcuate line.
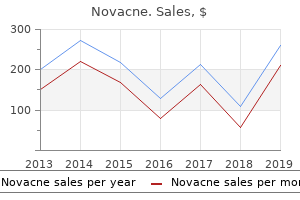
| Comparative prices of Novacne | | # | Retailer | Average price | | 1 | Dollar General | 746 | | 2 | Sports Authority | 884 | | 3 | Dollar Tree | 171 | | 4 | Walgreen | 127 | | 5 | Nordstrom | 449 | | 6 | Price Chopper Supermkts | 417 | | 7 | Family Dollar | 872 | | 8 | PetSmart | 650 | | 9 | Amazon.com | 476 | | 10 | Stater Bros. Holdings | 703 |
Cheap novacne online visaOcclusion of a branch of the central retinal vein normally leads to sluggish acne before and after discount novacne, painless loss of vision acne denim safe novacne 20mg. Accessory visible structures: the eyelids and lacrimal apparatus are protective devices for the eyeball. Extra-ocular muscle tissue: There are seven extra-ocular muscular tissues: four recti, two obliques, and a levator of the superior eyelid. Vasculature of orbit: Extra-ocular circulation is offered mainly by the ophthalmic (internal carotid) and infra-orbital (external carotid) arteries, the latter supplying structures close to the orbital ground. From a practical viewpoint, it would seem logical to discuss all three glands concurrently in affiliation with the anatomy of the mouth. However, from an anatomical viewpoint, notably in dissection programs, the parotid gland is normally examined with or instantly subsequent to the dissection of the face for full exposure of the facial nerve. Dissection of the parotid region must be accomplished before dissection of the infratemporal area and muscular tissues of mastication or the carotid triangle of the neck. The submandibular gland is encountered primarily during dissection of the submandibular triangle of the neck, and the sublingual glands when dissecting the floor of the mouth. The parotid gland is enclosed within a tough, unyielding, fascial capsule, the parotid sheath (capsule), derived from the investing layer of deep cervical fascia. Fatty tissue between the lobes of the gland confers the flexibility the gland will have to have to accommodate the motion of the mandible. The apex of the parotid gland is posterior to the angle of the mandible, and its base is expounded to the zygomatic arch. A transverse slice via the mattress of the parotid gland demonstrates the connection of the gland to the encompassing structures. The gland passes deeply between the ramus of the mandible, flanked by the muscle tissue of mastication anteriorly and the mastoid course of and sternocleidomastoid muscle posteriorly. The parotid duct turns medially at the anterior border of the masseter muscle and pierces the buccinator muscle. At the anterior border of the masseter, the duct turns medially, pierces the buccinator, and enters the oral cavity via a small orifice opposite the 2nd maxillary molar tooth. The auriculotemporal nerve and the good auricular nerve, a branch of the cervical plexus composed of fibers from C2 and C3 spinal nerves, innervates the parotid sheath. The postsynaptic parasympathetic fibers are conveyed from the ganglion to the parotid gland by the auriculotemporal nerve. Sympathetic fibers are derived from the cervical ganglia via the external carotid nerve plexus on the exterior carotid artery. Sensory nerve fibers move to the gland via the nice auricular and auriculotemporal nerves. Temporal Region the temporal area of the pinnacle contains the lateral space of the scalp and the deeper gentle tissues overlying the temporal fossa of the skull, superior to the zygomatic arch. The temporal fossa, occupied primarily by the upper portion of the temporalis muscle, is bounded. The lateral wall of the infratemporal fossa is formed by the ramus of the mandible.
Order cheap novacne on lineIn the absence of regular passive or dynamic help skin care md buy generic novacne 10 mg on-line, the plantar calcaneonavicular ligament fails to help the pinnacle of the talus skin care trends purchase novacne 10mg fast delivery. Consequently, the pinnacle of the talus displaces inferomedially and becomes prominent. As a end result, some flattening of the medial part of the longitudinal arch happens, along with lateral deviation of the forefoot. Flat ft are frequent in older individuals, notably in the occasion that they undertake much unaccustomed standing or acquire weight quickly, including stress on the muscles and growing the pressure on the ligaments supporting the arches. Talipes equinovarus, the frequent kind (2 per 1,000 neonates), involves the subtalar joint; boys are affected twice as often as women. The foot is inverted, the ankle is plantarflexed, and the forefoot is 1864 adducted (turned toward the midline in an abnormal manner). The main abnormality is shortness and tightness of the muscle tissue, tendons, ligaments, and joint capsules on the medial side and posterior side of the foot and ankle. Knee joint: the knee is a hinge joint with a variety of motion (primarily flexion and extension, with rotation increasingly possible with flexion). Tibiofibular joints: the tibiofibular joints include a proximal synovial joint, an interosseous membrane, and a distal tibiofibular syndesmosis, consisting of anterior, interosseous, and posterior tibiofibular ligaments. Ankle joint: the ankle (talocrural) joint is composed of a superior mortise, fashioned by the weight-bearing inferior surface of the tibia and the two malleoli, which obtain the trochlea of the talus. Joints of foot: Functionally, there are three compound joints in the foot: (1) the medical subtalar joint between the talus and the calcaneus, the place inversion and eversion occur about an indirect axis; (2) the transverse tarsal joint, the place the midfoot and forefoot rotate as a unit on the hindfoot round a longitudinal axis, augmenting inversion and eversion; and (3) the remaining joints of the foot, which permit the pedal platform (foot) to kind dynamic longitudinal and transverse arches. It is the management and communications middle in addition to the "loading dock" for the body. The head also consists of particular sensory receivers (eyes, ears, mouth, and nose), broadcast units for voice and expression, and portals for the intake of gas (food), water, and oxygen and the exhaust of carbon dioxide. The head consists of the mind and its protective coverings (cranial vault and meninges), the ears, and the face. The face includes openings and passageways, with lubricating glands and valves (seals) to shut a few of them, the masticatory (chewing) gadgets, and the orbits that house the visible equipment. Disease, malformation, and trauma of buildings within the head kind the bases of many specialties, together with dentistry, maxillofacial surgical procedure, neurology, neuroradiology, neurosurgery, ophthalmology, oral surgery, otology, rhinology, and psychiatry. The neurocranium is the bony case of the mind and its membranous coverings, the cranial meninges. It also accommodates proximal elements of the cranial nerves and the vasculature of the brain. The neurocranium in adults is shaped by a sequence of eight bones: 4 singular bones centered on the midline 1871 (frontal, ethmoidal, sphenoidal, and occipital), and two sets of bones occurring as bilateral pairs (temporal and parietal). It could mean the cranium (which includes the mandible) or the a part of the cranium excluding the mandible. There has additionally been confusion as a end result of some individuals have used the term cranium for under the neurocranium.
Discount novacneThe mesentery is a double-layered fold of visceral peritoneum that suspends the intestine and conducts neurovasculature from the posterior physique wall skin care 3m generic novacne 20 mg without a prescription. The mesentery is a fan-shaped fold of peritoneum that attaches the jejunum and ileum to the posterior belly wall acne grading scale buy generic novacne from india. The origin or root of the mesentery (approximately 15 cm long) is directed obliquely, inferiorly, and to the right. It extends from the duodenojejunal junction on the left aspect of vertebra L2 to the ileocolic junction and the right sacro-iliac joint. The common size of the mesentery from its root to the intestinal border is 20 cm. Between the 2 layers of the mesentery are the superior mesenteric vessels, lymph nodes, a variable amount of fat, and autonomic nerves. The transverse and sigmoid mesocolons and the mesentery of the jejunum and ileum 1101 have been cut at their roots. The ileocolic and proper colic arteries on the right facet and the left colic and sigmoid arteries on the left aspect initially coursed inside mesenteries (ascending and descending mesocolons) that later fused to the posterior wall; they can be re-established surgically. The arteries unite to form loops or arches, known as arterial arcades, which give rise to straight arteries, called vasa recta. Specialized lymphatic vessels in the intestinal villi (tiny projections of the mucous membrane) that absorb fat are called lacteals. They empty their milklike fluid into the lymphatic plexuses within the partitions of the jejunum and ileum. The lacteals drain in turn into lymphatic vessels between the layers of the mesentery. Within the mesentery, the lymph passes sequentially via three groups of lymph nodes. The superior nodes form a system by which the central nodes, at the root of the superior mesenteric artery, receive lymph from the mesenteric, ileocolic, right colic, and center colic nodes, which in turn receive lymph from juxta-intestinal lymph nodes. Efferent lymphatic vessels from the mesenteric lymph nodes drain to the 1103 superior mesenteric lymph nodes. Lymphatic vessels from the terminal ileum observe the ileal department of the ileocolic artery to the ileocolic lymph nodes. The sympathetic fibers in the nerves to the jejunum and ileum originate in the T8�T10 segments of the spinal wire and reach the superior mesenteric nerve plexus by way of the sympathetic trunks and thoracic abdominopelvic (greater, lesser, and least) splanchnic nerves. The presynaptic sympathetic fibers synapse on cell our bodies of postsynaptic sympathetic neurons within the celiac and superior mesenteric (prevertebral) ganglia. The parasympathetic fibers in the nerves to the jejunum and ileum derive from the posterior vagal trunks. The presynaptic parasympathetic fibers synapse with postsynaptic parasympathetic neurons in the myenteric and submucosal plexuses of the enteric nervous system in the intestinal wall (see additionally "Summary of Innervation of Abdominal Viscera," p.
Buy novacne 5 mg overnight deliveryPelvic Arteries the pelvis is richly equipped with arteries acne nodules order novacne online, among which multiple anastomoses happen acne under a microscope buy generic novacne 5 mg on-line, providing an extensive collateral circulation. The origins, programs, and distribution of the arteries and the 1340 arterial anastomoses fashioned are described in Table 6. Six main arteries enter the lesser pelvis of females: the paired inner iliac and ovarian arteries and the unpaired median sacral and superior rectal arteries. The ureter crosses the common iliac artery or its terminal branches at or instantly distal to the bifurcation. The inner iliac artery is separated from the sacro-iliac joint by the interior iliac vein and the lumbosacral trunk. It descends posteromedially into the lesser 1342 pelvis, medial to the exterior iliac vein and obturator nerve and lateral to the peritoneum. Although variations are widespread, the interior iliac artery normally ends on the superior edge of the larger sciatic foramen by dividing into anterior and posterior divisions (trunks). The branches of the anterior division of the interior iliac artery are primarily visceral. Anterior divisions of the internal iliac arteries normally provide a lot of the blood to pelvic buildings. Before birth, the umbilical arteries are the primary continuation of the interior iliac arteries, passing along the lateral pelvic wall after which ascending the anterior abdominal wall to and through the umbilical ring into the umbilical twine. Prenatally, the umbilical arteries conduct oxygen- and nutrient-deficient blood to the placenta for replenishment. When the umbilical wire is minimize, the distal parts of these vessels now not perform and turn out to be occluded distal to branches that pass to the bladder. The ligaments raise folds of peritoneum (medial umbilical folds) on the deep surface of the anterior abdominal wall (see Chapter 2, Back). Postnatally, the patent components of the umbilical arteries run antero-inferiorly between the urinary bladder and the lateral wall of the pelvis. It runs antero-inferiorly on the obturator fascia on the lateral wall of the pelvis and passes between the obturator nerve and vein. Within the pelvis, the obturator artery gives off muscular branches, a nutrient artery to the ilium, and a pubic branch. It ascends on the pelvic surface of the pubis to anastomose with its fellow of the opposite facet and the pubic department of the inferior epigastric artery, a branch of the exterior iliac artery. In a typical variation (20%), an aberrant or accent obturator artery arises from the inferior epigastric artery and descends into the pelvis along the standard route of the pubic branch. The extrapelvic distribution of the obturator artery is described with the decrease limb (Chapter 7). In females, it might occur-with almost equal frequency-as a separate department of the internal iliac artery or as a department of the uterine artery. The uterine artery is an additional department of the inner iliac artery in females, often arising separately and immediately from the internal iliac artery. It descends on the lateral wall of the pelvis, anterior to the internal iliac artery, 1344 and passes medially to attain the junction of the uterus and vagina, the place the cervix (neck) of the uterus protrudes into the superior vagina.
Effective novacne 5mgThe despair between these bones is converted by the pisohamate ligament into an osseofibrous tunnel skin care wholesale cheap 5mg novacne with amex, the ulnar canal (Guyon tunnel) acne used cash buy genuine novacne online. Ulnar canal syndrome (Guyon tunnel syndrome) is manifest by hypoesthesia (reduced sense of contact or sensation) within the medial one and a half fingers and weak spot of the intrinsic muscles of the hand. Handlebar Neuropathy People who experience long distances on bicycles with their arms in an prolonged place against the hand grips put pressure on the hooks of their hamates. This sort of nerve compression, which has been called handlebar neuropathy, results in sensory loss on the medial side of the hand and weak spot of the intrinsic hand muscles. Radial Nerve Injury in Arm and Hand Disability Although the radial nerve provides no muscle tissue within the hand, radial nerve injury within the arm can produce critical hand incapacity. The attribute handicap is incapability to extend the wrist ensuing from paralysis of extensor muscular tissues of the forearm, all of which are innervated by the radial nerve. The hand is flexed on the wrist and lies flaccid, a condition generally known as 646 wrist-drop (see the medical box "Injury to Radial Nerve in Arm"). The fingers of the relaxed hand additionally remain in the flexed position at the metacarpophalangeal joints. The loss of the ability to prolong the wrist affects the size pressure relationship of the wrist and finger flexors. The interphalangeal joints may be prolonged weakly through the motion of the intact lumbricals and interossei, which are provided by the median and ulnar nerves (Table 3. Thus, the extent of anesthesia is minimal, even in critical radial nerve injuries, and is normally confined to a small space on the lateral part of the dorsum of the hand. Dermatoglyphics the science of learning ridge patterns of the palm, known as dermatoglyphics, is a useful extension of the conventional physical examination of individuals with sure congenital anomalies and genetic illnesses. In addition, they often have a single transverse palmar crease (Simian crease); nevertheless, approximately 1% of the general population has this crease with no different medical features of the syndrome. Palmar Wounds and Surgical Incisions the placement of superficial and deep palmar arches ought to be saved in mind when inspecting wounds of the palm and when making palmar incisions. Furthermore, it is very important know that the superficial palmar arch is on the same stage as the distal end of the common flexor sheath. As talked about beforehand, incisions or wounds alongside the medial surface of the thenar eminence could injure the recurrent department of the median nerve to the thenar muscular tissues (see the clinical field "Trauma to Median Nerve"). Organization: the muscles and tendons of the hand are organized into 5 fascial compartments: two radial compartments (thenar and adductor) that serve the thumb, an ulnar (hypothenar) compartment that serves the little finger, and two more central compartments that serve the medial four digits (a palmar one for the long flexor tendons and lumbricals, and a deep one between the metacarpals for the interossei). Muscles: the best mass of intrinsic muscle tissue is dedicated to the highly cell thumb. Indeed, when extrinsic muscles are additionally considered, the thumb has eight muscular tissues producing and controlling the wide array of movements that distinguish the human hand. Vasculature: the vasculature of the hand is characterised by multiple anastomoses between each radial and ulnar vessels and palmar and dorsal vessels. Thus, blood is usually available to all components of the hand in all positions as properly as while performing functions (gripping or pressing) which may otherwise compromise especially the palmar constructions. Innervation: Unlike the dermatomes of the trunk and proximal limbs, the zones of cutaneous innervation and the roles of motor innervation are properly 648 outlined, as are functional deficits.
|